

This article is an advertorial sponsored by plus medica
The blueflow Venous Stent developed by plus medica GmbH & Co. KG received CE mark in early 2018, and has now been used in 60 patients at two centres in Europe. The stent utilises a woven nitinol design, which comes in different diameters and lengths to treat chronic venous outflow obstructions. The dedicated venous indication works as an extension stent, suitable for treatment below the inguinal ligament.

Woven nitinol design combines flexibility with radial force
Dr Michael Lichtenberg, head of the Interventional Angiology and German Venous Center at Klinikum Arnsberg in Arnsberg, Germany, performed the first procedure with blueflow earlier this year. Lichtenberg tells Venous News that one of the main advantages with the blueflow Venous Stent is its design: “A special characteristic of the nitinol woven design is that it is flexible, but with a strong radial force. We do not expect to see any stent fractures with blueflow.” He adds, “The woven design means we can place the stent exactly where it is needed, even in areas with high compression. It is particularly good for treatment below the inguinal ligament, as the stent gives high resistance to external force.”
Dr Nils Kucher (Clinic of Angiology, University Hospital Zurich, Zurich, Switzerland) agrees, saying “the blueflow stent is the only venous stent with a woven nitinol design, rather than steel alloy which compromises flexibility. A benefit of this design is therefore that it has the great combination of flexibility and a strong radial force. For many indications in the venous system we do need both. We need to have flexibility, especially in the groin area, but you also have the inguinal ligament there which means that sometimes with conventional laser cut stents, we have observed stent fractures. We believe that with the blueflow Venous Stent we can avoid stent fractures, because woven nitinol can handle the force of external pressure which a laser cut stent cannot. This is one of the big advantages, and why we believe that this stent is the best stent available for the external iliac vein and the common femoral vein.”

Follow-up data show good patency at four months
“We now have some follow-up data for the patients treated in Arnsberg,” Lichtenberg says, “and all stents that we implanted are still patent, with no reocclusion. We did not have any feedback from patients about problems with the stent; no discomfort or pressure. Our latest follow-up was at four months.”
Kucher, who has now treated 12 patients with the blueflow Venous Stent, says he has used the device in several different scenarios, some more complicated than others, but even with difficult cases of severe obstruction he has managed to achieve “beautiful results” with this stent. “This is still early stages, but both Lichtenberg and I believe the device is an enriching addition to venous stents.”
“The benefit for us”, Kucher expands, “is that we now have an option with great flexibility for certain areas like with an occluded common femoral vein, but it can also be used for compressed veins, e.g. due to cancer.” Lichtenberg and Kucher both mentioned the stent is not indicated for May-Thurner and further investigations are needed, however, Kucher notes that “for all other indications I think the blueflow is a great addition. In my opinion, there is not one stent that fits all venous disease. We have so many different indications, and of course this requires different stents, but I think in the future, this woven design will clearly have a place in the venous system.”
Case report 1
Dr Michael Lichtenberg
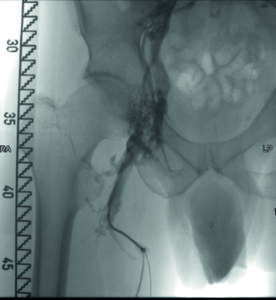
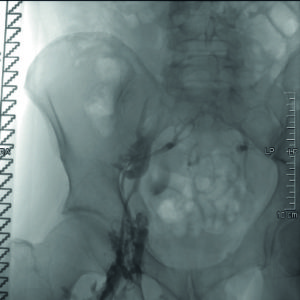
- A 44-year-old male patient with previous iliofemoral deep venous thrombosis of the right extremity, with persistent occlusion of the common femoral vein, external iliac vein and distal common iliac vein (Figures 1 and 2). Clinical symptoms included persistent swelling, lipodermatosclerosis and venous claudication (rVCSS 8, CEAP 4).
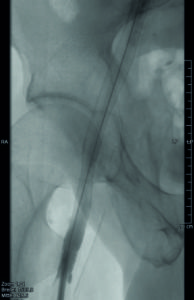
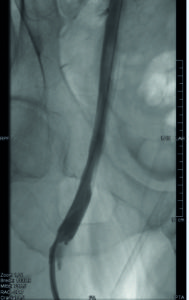
- After recanalisation with a 14mm balloon, two overlapping blueflow Venous Stents (14x150mm and 14x60mm) were implanted, demonstrating good inflow and outflow (Figures 3 and 4).
Case report 2
Dr Nils Kucher
- A 62-year-old male patient with leg swelling and venous claudication.
- He had a history of prostate cancer, tumour surgery and radiation therapy.
- A CT scan and venography confirmed compression of the external iliac and common femoral vein.
- After predilation with a 12mm balloon, a blueflow 14x100mm stent was implanted and then postdilated.
- Final venogram confirmed good stent apposition.
- The patients’ signs and symptoms of venous hypertension disappeared after the procedure.
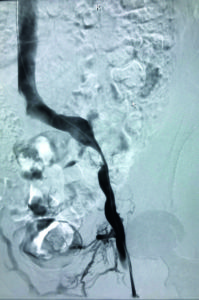
Figure 1: Baseline
venogram showing external iliac vein stenosis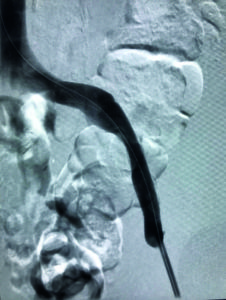
Figure 2: Final venogram of the implanted blueflow stent in the external iliac vein 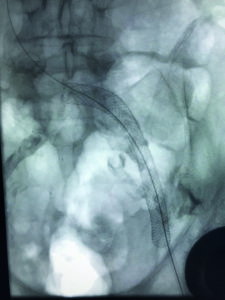
Figure 3: Fluoroscopic image of the implanted blueflow stent











